CVI symptoms are easy to dismiss as tiredness or “just getting older.” But chronic venous insufficiency affects an estimated 150 million people worldwide, and in the United States, up to 40% of women and 17% of men show some degree of chronic venous disease. Catching CVI early—before ulcers, clots, or irreversible skin changes occur—can dramatically change your outcome.
This guide explains what CVI disease symptoms actually look like at each stage, which risks demand urgent attention, and when it’s time to see a doctor for chronic venous insufficiency. If you’re near the Clear Lake–Webster–Kemah area of Texas, specialized vein care is closer than you think.
What Is Chronic Venous Insufficiency?
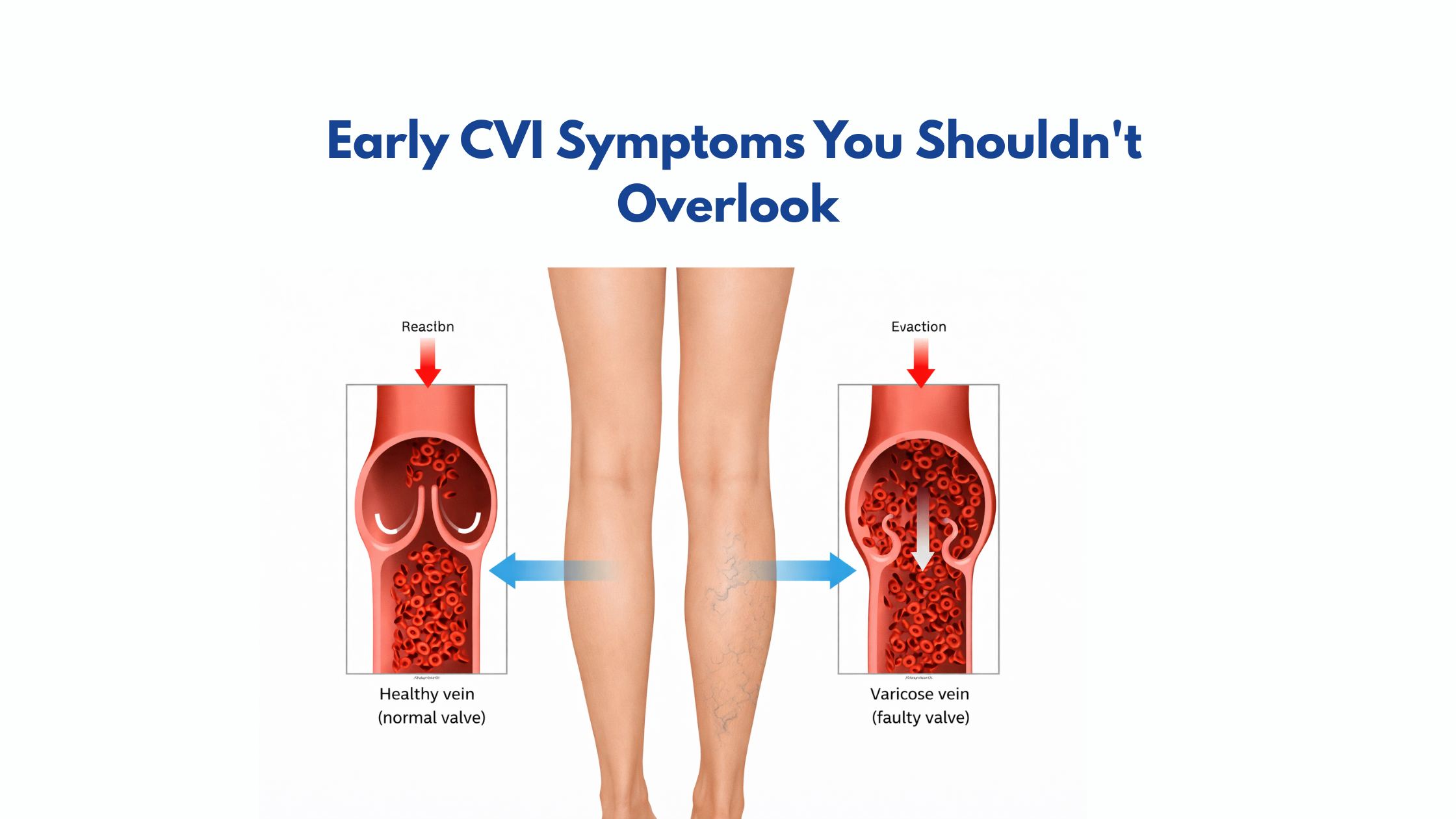
CVI occurs when the valves inside the leg veins weaken or fail. These valves normally act as one-way gates, pushing blood upward toward the heart. When they malfunction, blood pools in the lower legs, increasing venous pressure and triggering a cascade of CVI symptoms—from mild swelling to non-healing ulcers.
CVI is not the same as occasional tired legs or varicose veins, though those can be early warning signs. It is a progressive vascular condition that worsens without treatment.
Early CVI Symptoms You Shouldn’t Overlook
The earliest CVI symptoms are subtle and often mistaken for general fatigue or dehydration. Recognizing them early gives you the best chance of preventing progression.
- Leg heaviness or fatigue — especially after prolonged standing or sitting. The legs feel like they’re weighted down by the end of the day.
- Ankle swelling (edema) — particularly in the evening; socks leave deep indentations in the skin.
- Aching or throbbing in the calves — a dull, deep discomfort that is relieved by elevating the legs.
- Itching or tingling around the lower leg and ankle area, without an obvious skin rash.
- Visible spider veins or varicose veins — dilated, rope-like veins visible just beneath the skin surface.
- Skin changes near the ankles — redness, scaling, or darkening (hyperpigmentation) that may look like a rash or dry skin.
- Night cramps in the calves or feet often wake you from sleep.
Important: If you notice reddish-brown discoloration, hardening of the skin, or a sore that won’t heal near your ankle, these are advanced CVI signs. See a vein specialist or cardiologist in Webster TX immediately.
CVI Symptoms by Stage
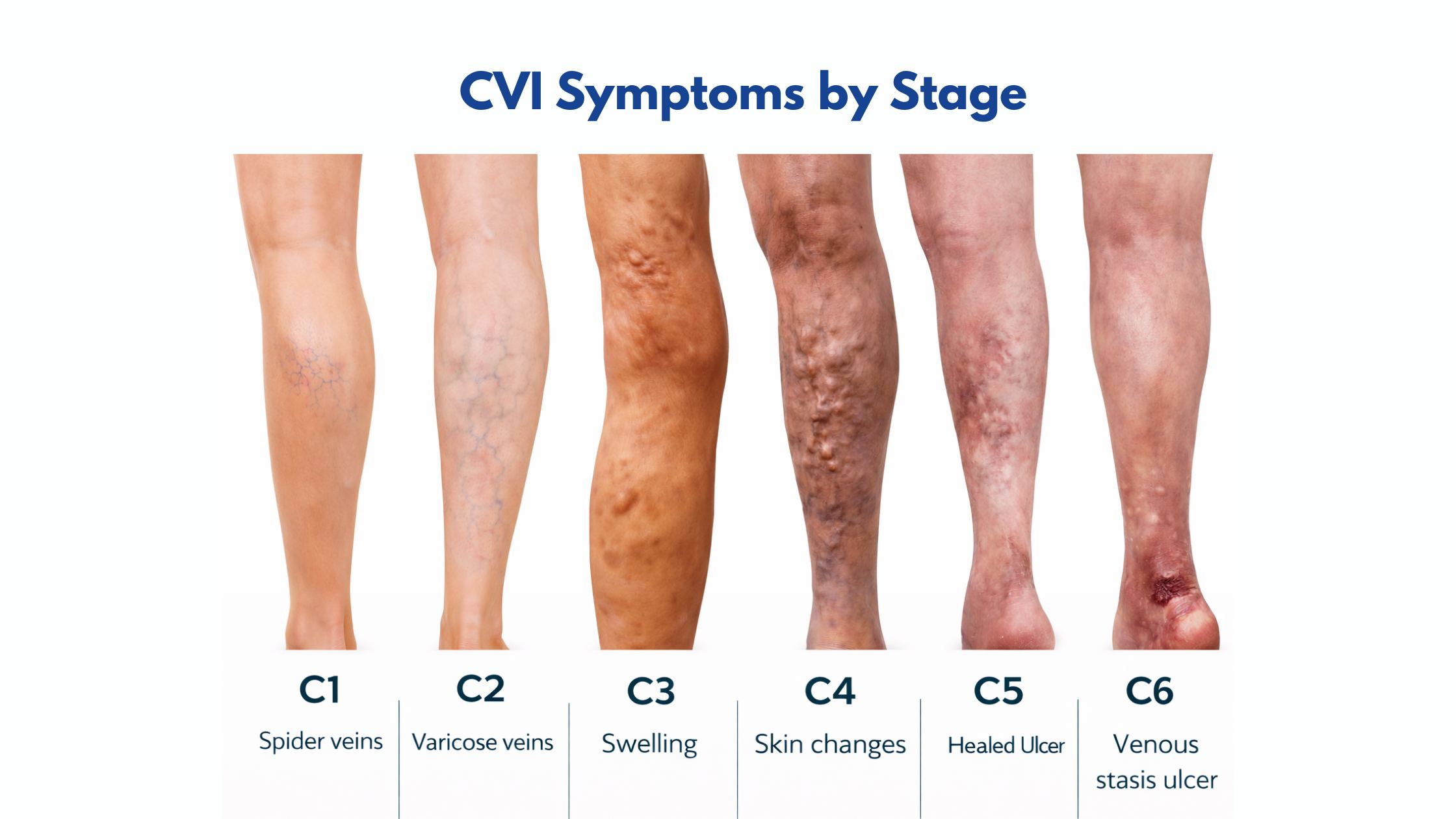
CVI is graded using the internationally recognized CEAP (Clinical-Etiology-Anatomy-Pathophysiology) classification. Understanding which stage you’re in helps your CVI doctor determine the most appropriate treatment.
| Stage | Visible Signs | Severity |
| C0 | No visible or palpable signs of venous disease | Minimal |
| C1 | Spider veins or reticular veins | Mild |
| C2 | Varicose veins ≥3mm in diameter | Moderate |
| C3 | Edema (swelling) without skin changes | Moderate |
| C4 | Skin pigmentation, eczema, lipodermatosclerosis | Advanced |
| C5 | Healed venous ulcer | Severe |
| C6 | Active open venous ulcer | Critical |
Most patients who come in for evaluation are at C2–C3, when CVI symptoms are uncomfortable but still highly treatable. Waiting until C5 or C6 significantly increases healing time and cost of care.
Can Chronic Venous Insufficiency Be Mistaken for Eczema?
Yes—and this misidentification happens more often than you might expect. A condition called venous stasis dermatitis (a direct consequence of advanced CVI) presents with redness, itching, flaking skin, and weeping patches around the inner ankle—nearly identical to atopic eczema on the surface.
The key difference: venous stasis dermatitis is caused by fluid leaking through capillaries due to high venous pressure. Treating it as simple eczema with topical steroids addresses the surface but ignores the underlying vascular problem. The American Academy of Dermatology recommends referral to a vascular specialist when eczema-like symptoms appear on the lower legs, especially if varicose veins or swelling are also present.
If you’ve been treating a “rash” near your ankle for months without improvement, it may be time to assess the underlying CVI.
Chronic Venous Insufficiency Risks: Who Is Most Vulnerable?

CVI doesn’t develop randomly. Certain factors significantly increase your likelihood of developing the condition or accelerating its progression:
- Age over 50 — Valve function naturally deteriorates with age
- Female sex — Hormonal changes (pregnancy, menopause) affect the vein wall elasticity
- Prior DVT or blood clots — Post-thrombotic syndrome is a major CVI risk factor
- Obesity — Increased abdominal pressure impedes upward venous return
- Sedentary lifestyle or prolonged standing — Both impair calf muscle pump function
- Family history of varicose veins or CVI
- Multiple pregnancies — Repeated increases in pelvic pressure damage venous valves
According to research, cardiovascular risk factors—including hypertension and metabolic syndrome—often overlap significantly with CVI, which is one reason a cardiologist’s perspective adds unique diagnostic value.
Is Chronic Venous Insufficiency Fatal? Understanding Prognosis
CVI itself is not typically fatal, and most patients with properly managed CVI maintain a normal quality of life and life expectancy. However, this question deserves a nuanced answer. Untreated or severely neglected CVI can lead to complications that carry real mortality risk:
- Deep Vein Thrombosis (DVT) — Blood clots that form in deep leg veins
- Pulmonary Embolism (PE) — A clot that travels to the lungs; potentially fatal
- Chronic venous ulcers — Open wounds that can become severely infected
- Cellulitis — Skin and soft tissue infections from a compromised skin barrier
A landmark study in the Journal of Vascular Surgery found that patients with active venous ulcers had significantly increased all-cause mortality, largely driven by concurrent cardiovascular disease. This reinforces why cardiovascular evaluation matters in CVI management.
The bottom line on chronic venous insufficiency prognosis: with early diagnosis and appropriate treatment, most patients do well. The survival rate for CVI is favorable when the underlying venous disease is addressed before complications arise.
Diagnosis of Chronic Venous Insufficiency: What to Expect

Diagnosis of chronic venous insufficiency combines clinical evaluation with non-invasive imaging. The process typically involves:
1. Clinical History and Physical Exam
Your CVI doctor will ask about symptom duration, family history, prior clots, and occupational habits. Physical examination assesses skin changes, varicose veins, edema, and the condition of the skin around your ankles.
2. Duplex Ultrasound
This is the gold-standard diagnostic tool for CVI. It uses sound waves to visualize blood flow in real time, detecting valve reflux (backward flow) and identifying any obstructions. The Society for Vascular Medicine recommends duplex ultrasound as the primary imaging modality for suspected CVI.
3. Additional Testing When Needed
In complex or advanced cases, venography, CT scanning, or intravascular ultrasound may be used to map deep venous anatomy before surgical intervention.
CVI Treatment Options

CVI treatment options range from lifestyle modification to minimally invasive procedures. The right path depends on your CEAP stage, CVI symptoms, and overall health.
1. Chronic Venous Insufficiency Self-Care (First-Line Measures)
- Compression therapy — Graduated compression stockings (20–30 mmHg or 30–40 mmHg) reduce venous reflux and edema.
- Leg elevation — Elevating legs above heart level for 30 minutes, 3–4 times daily, reduces pressure.
- Regular walking — Activates the calf muscle pump, the body’s most powerful mechanism for venous return.
- Weight management — Reducing BMI decreases abdominal venous pressure.
- Avoiding prolonged standing or sitting — Shift position every 30–45 minutes.
2. Medical and Minimally Invasive CVI Treatment Options
- Sclerotherapy — Injection of a chemical agent into small varicose or spider veins to collapse them.
- Endovenous Laser Ablation (EVLA) — Laser energy delivered inside the vein causes it to seal shut; highly effective for great saphenous vein reflux
- Radiofrequency Ablation (RFA) — Similar mechanism to EVLA using heat via radiofrequency waves
- VenaSeal — Medical adhesive injected to close the diseased vein without heat
- Phlebectomy — Surgical removal of bulging surface veins through tiny incisions
- Stenting — For obstructive CVI, a stent may be placed in the iliac vein to restore outflow
The Society for Vascular Surgery guidelines recommend thermal ablation (EVLA or RFA) as the preferred first-line intervention for great saphenous vein reflux, based on superior long-term outcomes compared to conventional surgery.
When to See a CVI Doctor
Many patients delay seeing a doctor for chronic venous insufficiency until CVI symptoms become severe. This is a costly mistake—both medically and financially. Schedule an evaluation with a chronic venous insufficiency doctor if you experience:
- Leg swelling that doesn’t resolve overnight with elevation
- Skin discoloration, hardening, or darkening around the ankle
- A wound or sore near the ankle that isn’t healing after 2 weeks
- Sudden worsening of pain, redness, or warmth in a leg (possible DVT—seek emergency care)
- CVI symptoms that are worsening despite compression stockings and self-care
The earlier CVI is caught, the more treatment options are available—and the better the outcomes. In most cases, minimally invasive office procedures can replace major surgery entirely.
Why Patients in Clear Lake, Webster & Kemah Trust Dr. Shalaby

For over 25 years, Dr. Shalaby—a board-certified cardiologist in Webster Texas—has been caring for the hearts and vascular health of patients across Clear Lake, Webster, Kemah, and surrounding communities. His clinical experience spans Texas Heart Institute, St. Luke’s Hospital, Clear Lake Regional Medical Center, Memorial Southeast Hospital, St. John Hospital, and Mainland Medical Center.
That breadth of hospital experience means Dr. Shalaby approaches vein disease with a cardiovascular lens—recognizing when CVI symptoms are a broader systemic issue that demands closer monitoring. Patients across these communities have access to world-class vein care without leaving the neighborhood they call home.
Summing Up
If you’ve recognized any of these symptoms, the next step is a professional vein evaluation. Dr. Shalaby’s vein center serves patients in Clear Lake, Webster, Kemah, and surrounding communities with personalized, evidence-based care.
To learn more about your chronic venous insufficiency treatment options or to schedule a screening for chronic venous insufficiency stages, visit our Vein Center or call us directly at 281-956-7070.