If your legs ache by mid-afternoon, swell after long days on your feet, or show rope-like varicose veins beneath the skin, you may be dealing with venous reflux disease — a condition affecting an estimated 40% of adults in the United States. Two procedures dominate modern treatment: sclerotherapy and laser ablation. Understanding the difference between Sclerotherapy vs Laser Ablation is the first step toward choosing the right path for your vascular health.
This guide walks through both Sclerotherapy vs Laser Ablation treatments in clinical detail: how they work, who qualifies for each, what the evidence says, and how a board-certified cardiologist determines the right approach for each patient.
What Is Venous Reflux Disease?

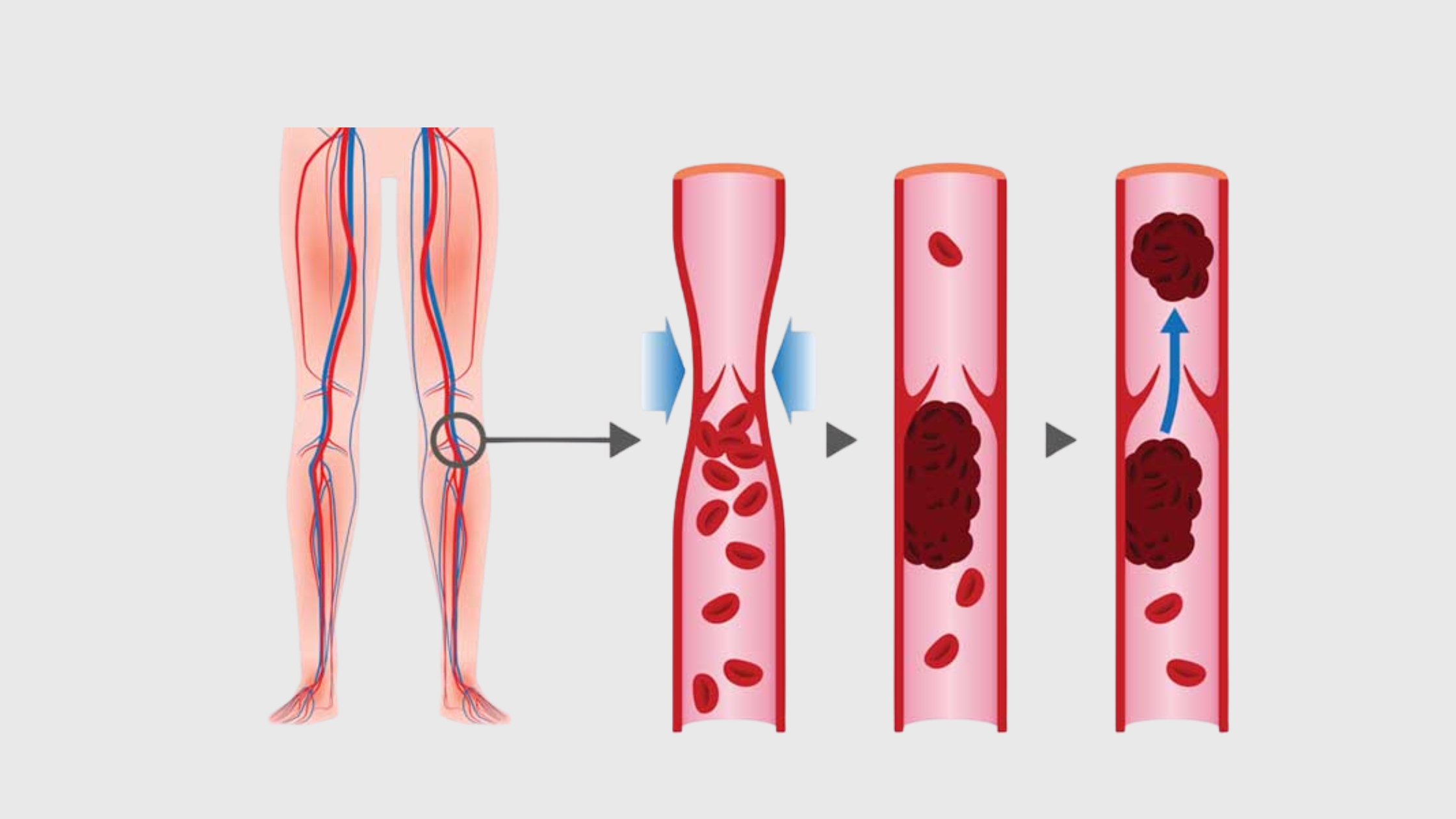
Veins carry blood from your extremities back to the heart. To do this against gravity, they rely on a series of one-way valves that open as blood moves upward and snap shut to prevent backflow. Venous reflux disease — also called chronic venous insufficiency — occurs when those valves weaken or fail.
When the valves don’t close properly, blood pools in the lower legs. Pressure builds. Over time, this produces a cascade of symptoms that range from cosmetic nuisance to serious medical complications.
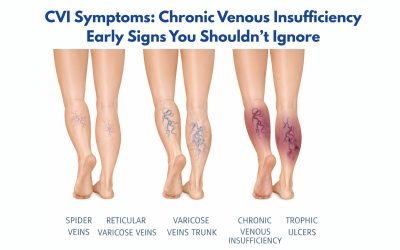
Common Symptoms by Stage
- Early stage: Spider veins, mild leg heaviness, occasional aching.
- Intermediate: Visible varicose veins, persistent swelling (edema), cramping, skin discoloration.
- Advanced venous reflux disease: Lipodermatosclerosis (skin hardening), chronic ulcers near the ankle, and significant mobility limitations.
Why is Early Treatment of Venous Reflux Disease Important?
Delaying venous reflux disease treatment can lead to worsening symptoms and complications. If left untreated, the risks include:
- Chronic swelling and discomfort
- Skin discoloration and thickening
- Venous ulcers
- Progression to advanced venous reflux disease
The National Institutes of Health highlights that early intervention improves outcomes and reduces long-term complications.
What Is Sclerotherapy? How It Treats Venous Reflux Disease

Sclerotherapy is one of the oldest and most well-documented minimally invasive vein treatments available. The procedure involves injecting a chemical agent — called a sclerosant — directly into the affected vein using a very fine needle.
The sclerosant (commonly sodium tetradecyl sulfate or polidocanol) irritates the inner lining of the vein wall, triggering controlled inflammation. The vein collapses, seals shut, and is gradually absorbed by surrounding tissue over several weeks. Blood is naturally rerouted through healthier adjacent veins.
Types of Sclerotherapy
- Liquid sclerotherapy: Standard injection, most effective for spider veins and very small reticular veins
- Foam sclerotherapy: The sclerosant is mixed with air to create a foam solution, increasing contact surface area — preferred for small-to-medium varicose veins
- Ultrasound-guided sclerotherapy: Uses real-time imaging to treat deeper veins not visible from the surface
What to Expect
Each session typically takes 15–45 minutes in a clinical setting. No anesthesia is required. Compression stockings are worn for 1–2 weeks post-treatment. Multiple sessions may be needed depending on the extent of the disease. Most patients see results within 3–6 weeks as treated veins fade.
Evidence note: A systematic review found sclerotherapy to be more effective than surgery for small varicose veins and comparable in outcomes to surgery for certain medium-caliber veins when performed by experienced practitioners.
What Is Laser Ablation Surgery for Venous Reflux Disease?

Endovenous laser ablation (EVLA) — commonly called laser ablation surgery — represents a significant advancement in how large, symptomatic varicose veins are treated. Rather than removing the vein surgically (as in traditional vein stripping), laser ablation closes the vein from the inside using precisely controlled heat energy.
A thin laser fiber is inserted into the vein through a small puncture, guided into position using ultrasound imaging. Once in place, the laser emits pulses of light energy that heat the vein wall. The wall contracts, collapses, and the vein is sealed permanently. The body gradually reabsorbs it over the following months.
The Procedure Step by Step
- Local anesthesia (tumescent anesthesia) is applied along the vein.
- A small incision is made at the entry point — typically at the knee or lower calf.
- A thin catheter and laser fiber are threaded into the great saphenous vein under ultrasound guidance.
- The laser is activated as the fiber is slowly withdrawn, sealing the vein from inside.
- The incision site is closed with a small bandage — no sutures required.
- Compression bandaging is applied immediately.
Most patients return to walking the same day. Full recovery takes 1–2 weeks. A follow-up ultrasound typically confirms successful closure at 2–4 weeks post-procedure.
Clinical data: According to a study in the Journal of Vascular Surgery, endovenous laser ablation achieves a technical success rate of 93–98%, with five-year recurrence rates significantly lower than surgical vein stripping. It has become the preferred first-line treatment of laser ablation doctors for great saphenous vein insufficiency.
Sclerotherapy vs Laser Ablation: Comparison

| Factor | Sclerotherapy | Laser Ablation (EVLA) |
| Best for | Spider veins, small–medium varicose veins | Large saphenous vein insufficiency, deep reflux |
| Anesthesia | None required | Local (tumescent) anesthesia |
| Procedure time | 15–45 minutes | 45–60 minutes |
| Sessions needed | 1–4+ sessions | Usually 1 session |
| Recovery | Immediate return to activity | Walking same day; full recovery 1–2 weeks |
| Treats deep venous reflux | Limited | Yes (primary indication) |
| Ultrasound guidance | Sometimes (foam UGFS) | Always |
| Success rate | ~80–85% (small veins) | ~93–98% (saphenous veins) |
| Insurance coverage | Often cosmetic (self-pay) | Often covered when medically necessary |
Which Venous Reflux Disease Treatment Is Better?

There is no one-size-fits-all answer. Whether Sclerotherapy vs Laser Ablation, the “best” treatment for deep venous reflux disease depends on:
- Size and location of affected veins
- Presence of deep venous reflux disease
- Symptom severity
- Overall vascular health
General guidance:
- Choose sclerotherapy for smaller, surface-level veins
- Choose laser ablation for deeper, symptomatic vein disease
In many cases, a combination of both Sclerotherapy vs Laser Ablation treatments in case of advanced venous reflux disease delivers optimal results.
How a Venous Reflux Disease Treatment Plan Is Actually Decided
The most common mistake patients make is assuming they need one treatment or the other. In practice, many patients require both — in sequence. A comprehensive treatment plan typically begins with a duplex ultrasound study to map the venous system and identify which veins are refluxing and at what depth.
The Diagnostic-to-Treatment Pathway
- Duplex ultrasound evaluation: Identifies the source and extent of reflux — essential before any procedure.
- Treat the source first: If the great or small saphenous vein is the primary source, laser ablation is addressed before superficial veins.
- Address residual veins: After the saphenous vein is closed, smaller tributary and spider veins are treated with sclerotherapy in follow-up sessions.
- Compression and monitoring: Ongoing compression therapy and follow-up ultrasound confirm results and monitor for recurrence.
Choosing the Right Specialist for Venous Reflux Disease Treatment
Selecting the right doctor for chronic venous insufficiency plays a critical role in the success of any venous reflux disease treatment. Because vein conditions can range from mild cosmetic concerns to complex circulatory disorders, expertise in both vascular and cardiovascular health is essential.
What to look for in a qualified doctor for chronic venous insufficiency:
- Board certification in cardiology or vascular medicine
- Experience with both sclerotherapy and laser ablation procedures
- Access to advanced diagnostic tools such as Duplex Ultrasound
- A comprehensive approach that evaluates overall circulation—not just visible veins
For individuals with moderate to advanced venous reflux disease, working with a certified cardiologist in Webster TX or laser ablation doctors who understands the connection between vein health and cardiovascular function can lead to more accurate diagnoses and better long-term results.
With over 25 years of experience serving communities such as Kemah, Clear Lake, and Webster, Dr. Shalaby brings a depth of clinical insight as a reputed doctor for chronic venous insufficiency shaped by his work in respected institutions, including the Texas Heart Institute and regional medical centers. Being a well-renowned cardiologist in Webster Texas, his approach emphasizes precise diagnosis, evidence-based venous reflux disease treatment, and patient-specific care planning.
Conclusion
Venous reflux disease is progressive. Left untreated, it doesn’t stabilize — it advances. This is where experience matters. As a board-certified cardiologist in Webster Texas with over 25 years of experience in venous reflux disease surgery, Dr. Shalaby brings a comprehensive perspective that connects vein health with overall cardiovascular function. For patients seeking clarity on the most appropriate treatment path, Dr. Shalaby can help with expert evaluation.
If you’re experiencing leg heaviness, varicose veins, or swelling, a duplex ultrasound evaluation is the right first step. Dr. Shalaby’s team serves patients from Clear Lake, Webster, Kemah, and surrounding communities with the expertise of a board-certified cardiologist in Webster TX. Visit The Vein Center or speak with our team directly at 281-956-7070.